
Table of Contents
We need to change how we schedule. Provider-time scheduling minimizes chaos and enables the flow state. Let’s dive in and see why.
Most clinic schedules look “full” and organized—until the day starts. It’s patient-time oriented and we think it’s fine.
Then reality shows up: multiple patients are dilated and ready at the same time, OCTs are stacked, IOP checks are waiting, consents are incomplete, and the physician is getting pulled in five directions. The schedule said it would work. The day feels like sprinting.
That disconnect is not a people problem. It’s a scheduling model problem.
The fix is simple to say and hard to adopt:
Stop scheduling around the patient’s total visit time. Start scheduling around the provider’s critical time. That means provider-time scheduling.
That idea has been used in dentistry for years (often called provider-time scheduling)—but most medical clinics still operate on a patient-time calendar. Ophthalmology is a perfect specialty to apply this because so much of the visit can (and should) be done by techs and diagnostics before the physician needs to step in
Why patient-time scheduling looks fine, but fails
What most schedules are built to do
Most practices (dental and medical) are running a version of chair-time scheduling, even if they don’t call it that. The schedule tracks:
- when the patient arrives
- how long they occupy a room/lane
- whether the day “fits” into physical space
It answers: “Can we fit these patients into rooms?”
It does not explicitly answer: “Where does the provider need to be at every moment?”
So the schedule can be “true” for patient flow—and still be false for provider reality.
Figure 1: A schedule that looks calm
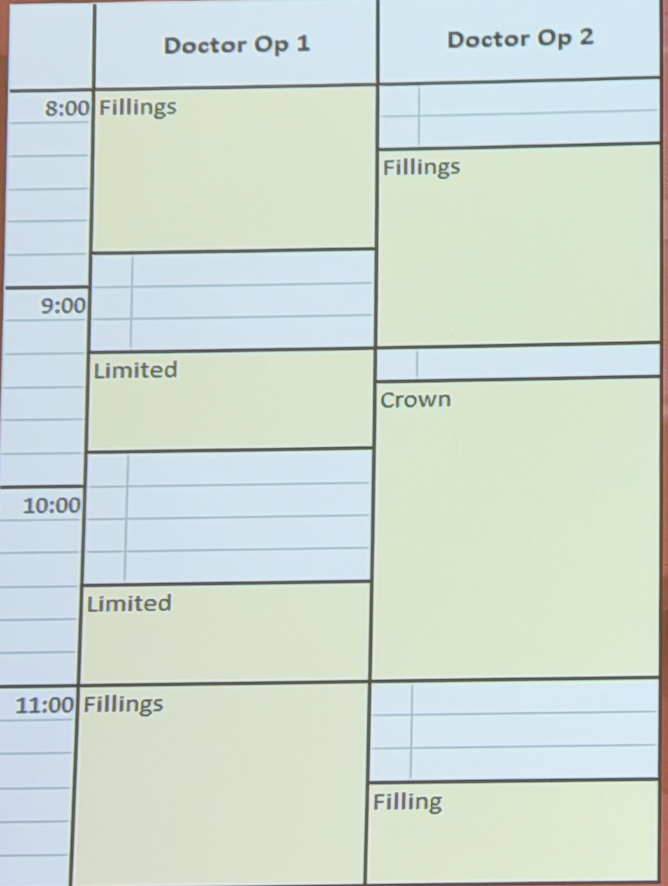
Let’s take a look at Figure 1 (a dental schedule, but the logic is identical to an ophthalmology lane schedule).
At first glance it looks calm. In OP1 (lane 1), there’s a patient at 8:00, then 9:20, then 10:30, then 11:00. In OP2 (lane 2), it also looks okay: a filling at 8:20, a crown at 9:30, and another filling at 11:30.
No overlap, right?
But this view is patient-time. It tells you where the patient is—not where the provider must be.
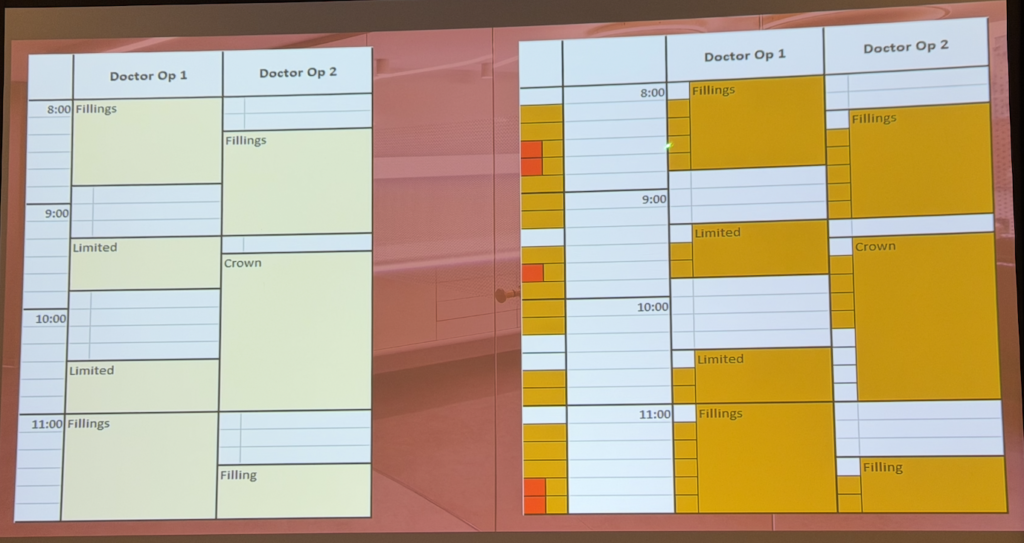
Figure 2: The schedule underneath the schedule. The missing layer: provider-critical time
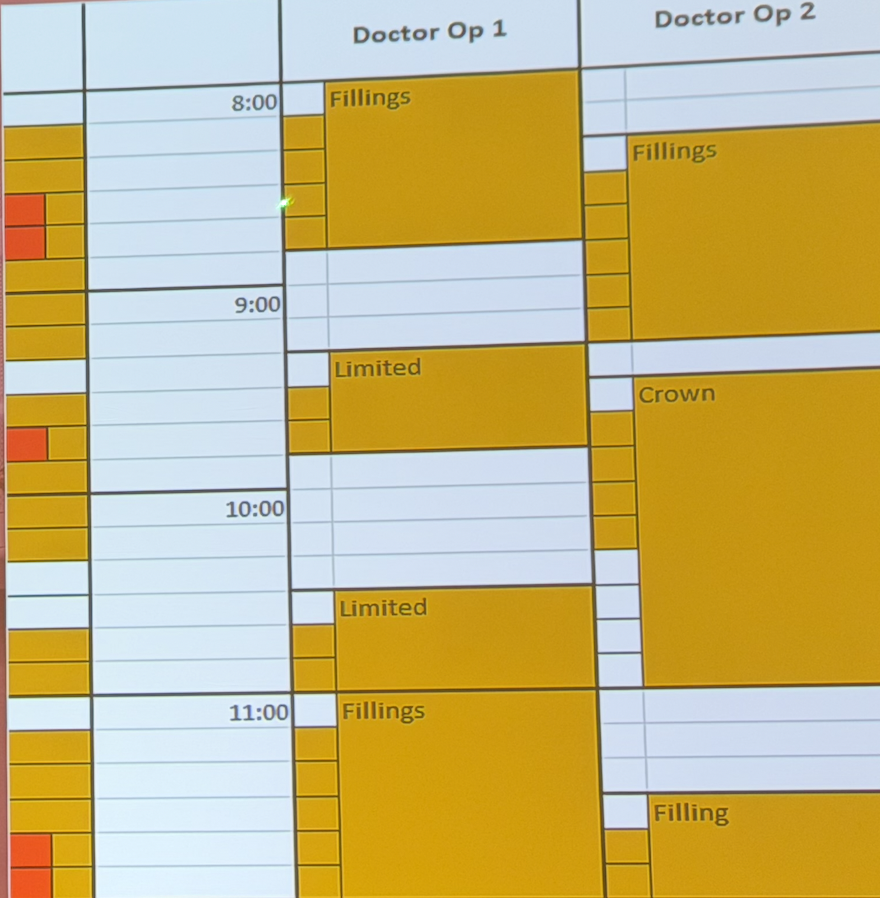
Now look at Figure 2, which analyzes Figure 1 by mapping provider-critical time. The orange blocks represent the minutes when the doctor must be present.
- OP1: provider needed 8:10–8:50, 9:30–9:50, 10:40–11:00, and 11:10–12:00
- OP2: provider needed 8:30–9:20, 9:40–10:20, and 11:40–12:00
Now ask the only question that matters:
Can one provider be in two rooms at once?
That’s where the chaos comes from—not because the team is “slow,” but because the calendar is accidentally demanding the impossible.
Why the current model creates stress even when you’re “fully staffed”
Once you map provider-time, you see the real pattern: Look back to figure 2.
- Red blocks = provider double-booked
- White blocks = provider idle / underutilized time created by mismatched flow
What looked calm in Figure 1 becomes a stop-start day in Figure 2:
- smooth from 8:00–8:30
- double-booked and rushed 8:30–8:50
- smooth 8:50–9:20
- idle 9:20–9:30
- smooth 9:30–9:40
- double-booked 9:40–9:50
- smooth 9:50–10:20
- idle 10:20–10:40
This is why a “normal” schedule can feel chaotic: patient-time scheduling hides provider collisions and forces constant context switching.
And that context switching is the real tax.
Patients notice the chaos, and this leads to poor experiences.
Flow state is the hidden engine of speed
Most practices unintentionally build a HIIT day for the doctor: sprint → stop → sprint → stop.
Even when each interruption is “only a minute,” the total switching tax is enormous: move rooms, reorient, review chart, sanitize, knock, re-explain, re-focus, and restart.
- In dentistry: flow state is staying with one patient in one room while the assistant is perfectly in sync—handoffs are automatic and steps happen back-to-back—and it gets broken the moment you leave the room because you must reset before you can work again.
- In ophthalmology: flow state is a steady rhythm of moving smoothly from patient to patient with testing already staged—review data, examine, decide, consent, treat—and it gets destroyed when you bounce rooms because every exit forces a restart (chart review, knocking, hand hygiene, re-explaining, re-focusing), which quietly adds minutes and breaks momentum.
Flow isn’t a vibe. It’s a measurable operational advantage:
- fewer resets
- fewer repeated explanations
- fewer missed steps
- faster completion
- better patient experience
The current scheduling model breaks flow by design.
The injection visit that exposes the flaw
Let’s take a common scenario: an in-office injection.
Assume the total visit is one hour. In many clinics, the ophthalmologist does not need to be present for minute 0–45 because the tech-driven and diagnostic sequence includes:
- vision + interval history
- IOP
- dilation (plus waiting time)
- OCT / imaging
Only then does the physician need to: review scans, examine/verify, finalize plan, confirm consent, and perform the injection.
In other words:
- the patient is in the clinic for 60 minutes
- the doctor may only be needed for ~10 minutes—often around minute 45–55
The scheduling mistake
Most clinics schedule this as:
8:00–9:00 Injection Visit (patient-time block)
That optimizes the patient’s slot. It does not optimize the physician’s day.
So while your injection patient is waiting to become “doctor-ready,” another patient (say a glaucoma follow-up in lane 2) hits their own provider-critical window… and the collision happens. Staff starts chasing the MD. The day turns into red blocks.
The better approach
If the ophthalmologist truly needs to be there from 45–55, the schedule should be built around 45–55.
Plan the day as a sequence of physician-critical windows:
- Patient A: 8:45–8:55
- Patient B: 8:55–9:05
- Patient C: 9:05–9:15
Meanwhile techs and diagnostics run upstream so each patient becomes doctor-ready at the right time—without collisions.
This is provider-time scheduling in ophthalmology:
- schedule the provider’s required minutes
- align them into a steady rhythm
- let tech work happen before and after
Optimize the doctor’s time with provider-time scheduling, not the patient’s time (and why patients still win)
This sounds counterintuitive until you accept one truth:
The provider is the bottleneck resource.
If you optimize around the bottleneck, the whole system stabilizes.
When you schedule provider-critical time correctly:
- patients wait less at the end of visits
- techs stop stalling with “ready patients” and no doctor available
- procedures happen with less rushing
- the clinic stops feeling like it’s constantly behind
Paradoxically, scheduling around the doctor’s timeline often improves the patient experience more than “patient-time optimization” ever did—because patients mainly care that:
- the visit is predictable
- the physician is present when it matters
- they aren’t sitting “ready-and-waiting” with anxiety rising
The “rocks, sand, water” trap in ophthalmology (and why it breaks)
In ophthalmology, many clinics have accidentally adopted a “rocks, sand, water” approach—without realizing it. We anchor the day with big “rock” visits that consume large chunks of patient-time on the schedule, like a cataract consult or a comprehensive annual exam. Then we sprinkle in “sand” visits, like a retina follow-up for diabetic macular edema (often scheduled as a 30-minute dilation + OCT slot). And finally we squeeze in “water” visits—quick check-ins like a dry eye follow-up booked as 15 minutes.
The fallacy isn’t the categories. The fallacy is how we size them.
These blocks are usually built from the patient’s perspective—how long the patient is in the clinic—not from the provider’s perspective—how long the ophthalmologist is actually required. And in real clinic life, the time demands often flip the script: the “quick” dry eye visit can require more physician time (history nuance, counseling, exam decisions, treatment escalation), while a “bigger” retina follow-up may require surprisingly little physician time once testing is staged (VA/IOP/dilation/OCT completed, images ready, injection decision is straightforward).
Rock-sand-water can work—but only if those categories are defined by provider-time, not patient-time.
Buffer isn’t waste—it’s what keeps you on time
One fear with provider-time scheduling is: “What if something runs long?”
Something will run long. That’s normal.
The solution isn’t to pretend variability doesn’t exist. The solution is to build intentional buffer into provider templates so the day can absorb:
- late arrivals
- complex exams
- unexpected findings
- consent delays
- anxiety, questions, and real human time
And when things go smoothly, you don’t automatically cram more in. You use that buffer to document properly, communicate better, reset, reduce staff stress, and keep the afternoon from unraveling.
A schedule with zero slack isn’t efficient. It’s fragile.
Stop saying “fill the schedule” every week—build a two-mode system instead
If you tell your team “fill the schedule” every week, it becomes background noise. Nobody changes their behavior on Tuesday because they’ve heard the same message every Monday—so the phrase stops functioning as a real instruction.
Scott’s fix is a simple two-mode system with a clear trigger:
- Set a mandatory weekly minimum (a floor) using your real historical numbers—pick a number you naturally hit about 3 out of 4 weeks.
- If you’re above the floor: run normal. Protect flow. Don’t cram extra just to “grow.”
- If you’re below the floor: flip into planned all-hands mode for 1–3 days—reactivation calls/texts, short-notice fills, same-day conversion focus, targeted schedule work, and physician flexibility—until the week is back above the minimum.
Punchline: don’t squeeze already-full weeks (burnout risk for little gain). Fix the weak weeks. Then once the floor is consistently easy, raise the floor.
Putting it all together: transition from patient-time to provider-time scheduling
You don’t need a revolutionary tool. You need a different question:
“Where does the ophthalmologist need to be at every moment?”
Step 1: Break common visit types into phases
For each high-volume visit type (injection, glaucoma follow-up, retina eval, post-op, etc.), define:
- tech/diagnostic start
- diagnostic sequence
- provider-critical window
- wrap-up/discharge
Step 2: Build provider-time templates (per physician if needed)
Different physicians run at different speeds. That’s normal. Systemize it.
Example:
- Dr. A (faster): MD window :45–:55
- Dr. B (slower): MD window :45–:60
If you force Dr. B into Dr. A’s template, the chaos returns. Dr B b
Step 3: Train one non-negotiable rule
Never double-book provider time.
If you break this rule, you rebuild the chaos you’re trying to escape.
Step 4: Pilot, measure, refine
Start with one clinic session or one template for 2–4 weeks, then adjust based on real flow.
Flow is Foundation. Grow, Adapt, Optimize
Market to generate patient leads. Use tight phone scripts to get them scheduled. Schedule around provider time so the clinic never descends into chaos.
Our next post will focus on clinical case acceptance (and how it connects to financial commitment), and if you haven’t yet, go review the phone scripts post so you can schedule with precision and convert demand into a calm, predictable day.

Pingback: How to Improve Clinical Acceptance in Ophthalmology
Pingback: Financial Case Acceptance: The One-Sheet Script That Works