
Table of Contents
Watch this poorly executed financial case acceptance.
Picture this: a patient just finished a cataract consult.
They’ve heard the doctor explain what’s going on, they’ve seen the imaging, and they’re emotionally aligned with doing the right thing. They’re thinking:
“Okay… I guess we should fix this.”
Then we walk them to the next step and hand them… a software printout.
A page full of CPT codes, modifiers, test names, columns of estimates, “allowed amounts,” “deductible remaining,” line items, and enough numbers to make a CPA sweat.
And we’re surprised when they say:
- “Can I think about it?”
- “I need to talk to my spouse.”
- “Let me call my insurance.”
- “I’ll schedule later.”
It’s not because they suddenly stopped caring about their vision.
It’s because we accidentally triggered the most predictable human response in business:
Confusion makes buyers back away from commitment.
Ophthalmology—especially cataract, glaucoma, refractive, and dry eye—is one of the easiest places to accidentally create that confusion. And it’s one of the easiest places to fix it.
This post is a deep dive into why the typical financial presentation fails, what it’s doing to your schedule and cash flow, and how to replace it with a one-sheet format that’s built for how patients actually decide.
The Real Problem Isn’t Price. It’s Cognitive Load.
Most practices assume patients decline because the treatment is expensive.
Sometimes that’s true. But in day-to-day reality, the bigger killer is cognitive overload—especially in healthcare, where the patient already feels uncertain.
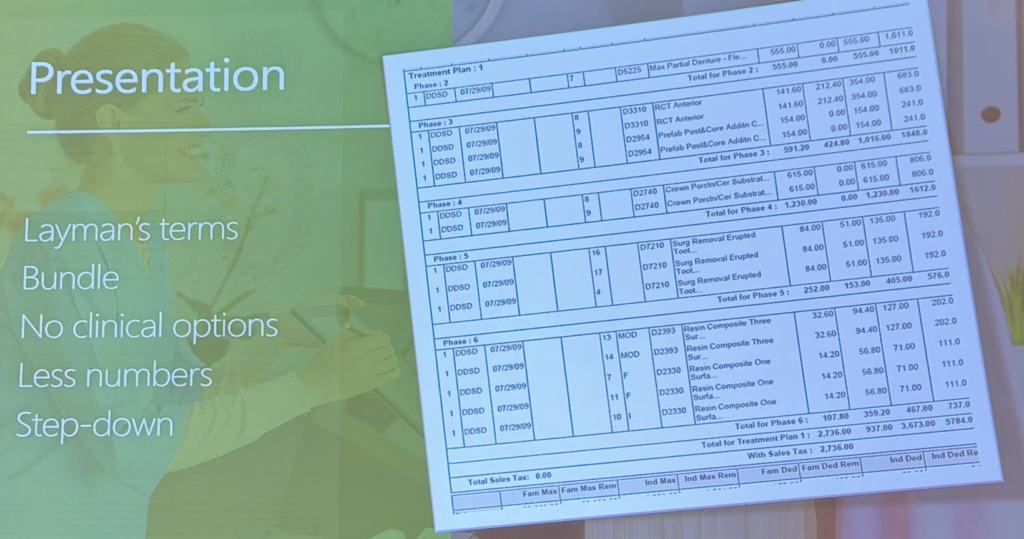
When you give someone an itemized “billing-style” estimate (like in figure 1), you create three decision problems at the same time:
- A comprehension problem
“I don’t understand what any of this means.” - A trust problem
“If I don’t understand it, how do I know it’s fair?” - A decision problem
“If I can’t evaluate it, I should delay.”
Delay is a rational response to uncertainty.
And healthcare software printouts are uncertainty machines.
Why Itemized Printouts Trigger the Worst Version of the Patient Brain
Let’s name the psychological mechanisms at play. This matters because if you understand the mechanism, you stop trying to “over-explain” your way out of it.
1) Choice overload: too many micro-decisions
An itemized estimate turns one decision (“Do I do this plan?”) into twenty decisions (“Do I want this line item? That test? This lens? That upgrade?”).
The brain hates that. It reacts by either:
- postponing, or
- negotiating random components (often in clinically dumb ways)
This is where you get the classic:
- “Can we do the surgery but skip the testing?”
- “Can we do the cataract but not the lens part?”
- “Can we do one eye and see if I like it first?” (sometimes valid clinically, often a stall tactic financially)
When you itemize, you invite cherry-picking.
2) “Step-up” pricing: patients mentally climb to the scariest number
Line items force patients to add… and add… and add… until they hit the largest total.
That means the moment you want them to commit is the moment they feel the most sticker shock.
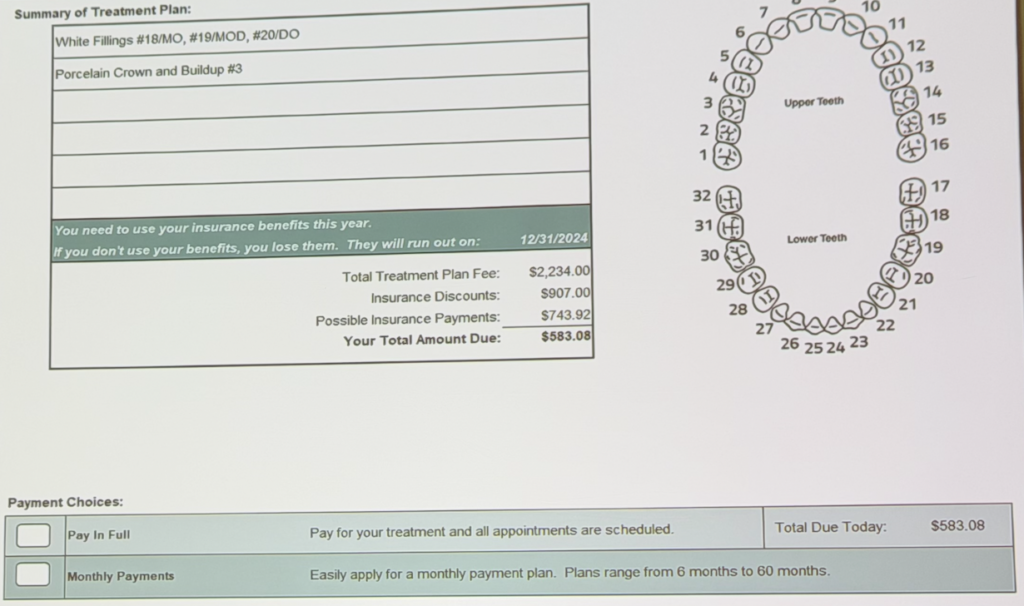
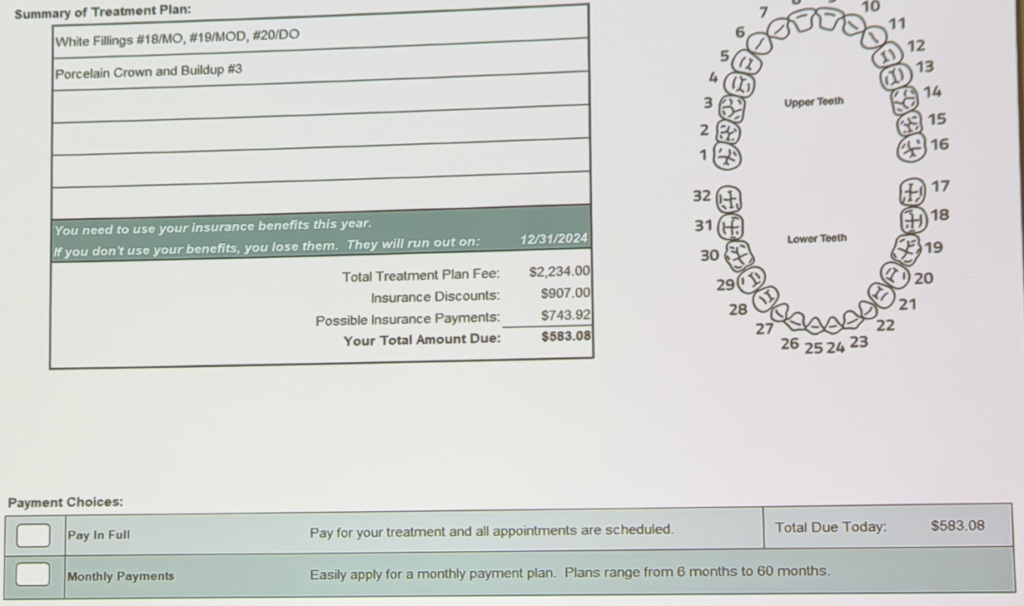
A better structure is step-down framing: See figure 2.
- total cost → adjustments/discounts → estimated insurance payment → patient portion
The patient lands on the commitment number after they’ve already experienced the relief of the step-down.
3) Precision bias: the penny makes it feel like a promise
“Estimated insurance payment: $742.46”
That looks scientific. It feels guaranteed. Patients anchor on it.
Then insurance pays $600 (or denies a component), and the patient feels betrayed—even if you included a disclaimer.
Humans don’t emotionally process disclaimers the way practices think they do.
They process the number you printed.
4) The “research trigger”: complexity tells them they must research
This is the same reason people walk out of a store when the salesperson hits them with five technical choices.
If the explanation feels like a foreign language, the patient concludes:
“I need to research this before I commit.”
In healthcare, “research” often means:
Google, friends, Facebook groups, insurance phone trees, and five weeks of delay.
Why Ophthalmology Gets Hit Harder Than Dentistry
Ophthalmology has built-in complexity that makes sloppy financial communication especially damaging:
- Cataract surgery has covered vs non-covered components (especially with upgrades)
- Facility vs professional billing confuses even smart patients
- Testing and imaging creates “why am I paying for diagnostics?” reactions
- Medicare compliance requires forms that can look like sales documents if mishandled
- Two-eye timelines (and multiple post-ops) creates more scheduling friction
- Glaucoma care has long-term risk language that patients don’t “feel” today
- Dry eye often lives in the gray zone between “medical necessity” and “value program”
Translation: ophthalmology patients are already a little uncertain.
Your financial presentation should reduce uncertainty, not multiply it.
The Key to Solid Financial Case Acceptance. Separate Claims Paperwork From Decision Paperwork
Here’s the most important mindset shift:
Your EHR/practice management printout is for claims.
Your patient-facing financial summary is for decisions.
They are not the same document. They should not look the same. They should not feel the same.
When you merge them, you create a Frankenstein page that satisfies nobody:
- It’s too confusing for the patient
- It’s too incomplete for compliance
- It’s too slow for your staff
- It’s too fragile for collections
The replacement is what I’ll call the:
One-Sheet Care Plan & Investment Summary
The one-sheet has one job, and figure 2 does this extremely well so reference it.
Help a normal person confidently say “yes” (or “not yet”) without confusion.
It needs five components:
1) The plan in plain English
Not codes. Not abbreviations. Not internal procedure names.
Examples:
- “Cataract surgery (right eye) with lens implant”
- “Cataract surgery with astigmatism correction upgrade”
- “Glaucoma laser procedure (SLT)”
- “Dry eye treatment program (90 days)”
- “Upper eyelid surgery”
- “LASIK (both eyes)”
2) One sentence on timing (not a lecture)
Just enough urgency to prevent drift.
- Cataract: “We want to schedule before your vision impacts driving and daily activities further.”
- Glaucoma: “We want to reduce pressure to lower risk of progression.”
- Dry eye: “This is best treated as a program—consistent steps over the next 8–12 weeks.”
3) Four numbers, maximum
The entire magic is that it’s not 40 numbers.
- Total fee (your standard fee)
- Contracted/plan adjustments (if applicable)
- Estimated insurance payment (clearly labeled as estimate)
- Estimated patient portion
That’s it.
4) Two options only
This is where most practices accidentally sabotage themselves by offering five financing explanations and three payment structures. Don’t.
Offer:
- Option 1: Take care of the patient portion today (or deposit today)
- Option 2: Monthly plan approved today / agreement signed today
The patient’s brain experiences this as: yes or yes.
5) A commitment rule (the part that changes your schedule immediately)
No “honor system” scheduling for high-value blocks.
Your rule becomes:
- “We schedule once we complete the financial arrangement today.”
That’s not aggressive. That’s normal commerce.
Airlines don’t hold seats without a ticket.
Surgery slots are seats.
What This Sounds Like Out Loud (Ophthalmology Scripts)
The tone matters as much as the format.
The highest-performing delivery is usually:
- short
- neutral
- logistical
- confident
- not apologetic
- not salesy
Because long emotional explanations feel like persuasion—which triggers defensiveness.
Cataract surgery: standard
“Mr. Jones, Dr. ___ recommends cataract surgery on your right eye. Let me go over the financial piece quickly so we can get you scheduled.
The total fee is ___. With your insurance adjustments and estimated insurance payment, your estimated portion is ___.
You have two options: option one is you take care of the ___ today and we lock in the surgery date. Option two is we set up a simple monthly plan today and we lock in the date. Which works better for you?”
Cataract + premium upgrade
Mr. Jones, as you heard Dr. Tran recommend, we’re planning cataract surgery with the lifestyle lens option we discussed to reduce how much you rely on glasses.
The cataract surgery itself is billed through your medical insurance. The lens upgrade portion is elective and not covered.
For the plan you chose, your estimated portion today is ___.
You’ve got two options: option one is you take care of the ___ today and I’ll lock in all your appointments. Option two is we set up a simple monthly plan today and I’ll lock in everything. Which is better for you?”
Notice what’s missing:
No deep explanation of Medicare rules, no multi-minute financing monologue, no “let me educate you on your deductible.”
If they ask, you answer. But you don’t pre-load risk and complexity.
The Hidden Operational Payoff: This Isn’t Just “Case Acceptance.” It’s Schedule Control.
A lot of practices think this is a “sales technique.”
It’s not. It’s operations.
When you require a financial commitment before scheduling:
You reduce no-shows and cancellations
Patients who commit financially behave differently than patients who “promised to come back.”
Not because they’re bad people—because human behavior follows commitment.
You cut checkout friction in half (or more)
If the financial piece is handled once, up front:
- fewer checkout touches
- fewer awkward payment moments on procedure day
- fewer “surprise” conversations that derail flow
- less staff time chasing balances
You protect your most expensive inventory: surgeon time
In ophthalmology, a broken surgery block is extremely costly:
- staffing
- facility coordination
- lens ordering/logistics
- pre-op testing windows
- patient transportation planning
Your scheduling policy should reflect that reality.
“But What About Medicare/ABNs/Compliance?”
This is where practices get stuck: they confuse simplicity with sloppiness.
You can be simple with patients and still be compliant.
The key is separation:
- One-sheet summary = decision tool
- ABN / required notices / upgrade agreements = compliance tool
Don’t make the ABN your sales deck.
Don’t lead with forms that feel like legal traps.
Use them when appropriate, after the patient understands the plan.
Also: be careful with wording. You’re not “warrantying outcomes.” You’re defining coverage, program structure, or what’s included.
(Not legal advice—just the operational principle that patient clarity and compliance paperwork are two different jobs.)
What If the Plan Changes After They Pay?
It will. This is medicine.
A clean system has a clean rule:
- If treatment is reduced: refund/credit promptly
- If treatment expands: pause, re-present the updated plan, get agreement, then proceed
The mistake is pretending plans never change.
The fix is building a workflow where changes are normal and handled cleanly—without turning every case into a billing debate.
The Ophthalmology Version of “Warranty” (Without Promising Outcomes)
In dentistry, “warranty” often means “if it breaks, we fix it.”
In ophthalmology you can’t ethically market a guarantee of vision, and you shouldn’t try.
But the underlying patient psychology still applies: patients hate future surprise costs.
So the equivalent is clarity about what’s included:
- Post-op visits included (define timeframe)
- Enhancement policy for refractive procedures (clear terms, clear limits)
- Dry eye programs packaged by phases (deliverables defined)
This reduces fear, reduces disputes, and lowers friction without making outcome promises.
Why This Works So Fast (Even in High-Dollar Cases)
People assume simplicity only works for small cases.
In reality, the bigger the case, the more the patient needs:
- fewer numbers
- clearer structure
- less “Google homework”
- fewer micro-decisions
One-sheet, plain-English, two-option financing works at:
- $500
- $5,000
- $25,000
- $70,000
Because it’s not a “cheap plan.”
It’s a clear plan.
How to Implement This Without Turning It Into a Six-Month Project
If you want this to change behavior immediately, the sequence matters.
Step 1: Build 3–5 one-sheet templates
Start with your highest-volume friction points:
- Cataract standard
- Cataract upgrades
- SLT / glaucoma procedure pathway
- Dry eye program (if you offer it)
- Oculoplastics / refractive (if applicable)
Step 2: Train on the 20-second delivery
Not the “explain everything you know” delivery.
Train for:
- speed
- neutrality
- confidence
- two options only
Step 3: Enforce the commitment rule consistently
If you apply it sometimes, patients learn to negotiate around it.
Consistency is what makes it feel normal.
Step 4: Track the metrics that prove it worked
Watch these for 2–4 weeks:
- consult → scheduled conversion rate
- cancellation/no-show rate (especially procedures/surgery)
- staff time spent in financial conversations
- number of payment touches per case
- A/R aging and patient balance volume
- upgrade conversion (if relevant)
When it’s working, you’ll feel it operationally:
- smoother flow
- fewer long phone calls
- fewer “insurance debates”
- fewer awkward checkout moments
- fewer schedule holes
The Bottom Line
Ophthalmology doesn’t need more sophisticated financial presentations.
It needs less—delivered better.
Patients don’t say yes because they saw 37 line items.
They say yes because they understood:
- what they need
- why now matters
- what it will cost them
- what their two next-step options are
If your current process forces patients to decode a billing statement in order to choose a medical plan, you’re not “being transparent.”
You’re outsourcing clarity to confusion.
And confusion always collects a tax—on case acceptance, on scheduling stability, and on your team’s time.
Focus on phones. Focus on scheduling right. Focus on clinical case acceptance. Then you can have higher case acceptance.
