
Table of Contents
Case acceptance is both financial and clinical acceptance.
Case acceptance is the percentage of patients who (1) understand the diagnosis, (2) believe treatment matters, and (3) take the next clear step—schedule, start treatment, or commit to a plan.
In ophthalmology, patients still delay or disappear because so much of eye care is either silent (glaucoma), slow (diabetic retinopathy), or elective-but-life-changing (cataracts, premium IOL choices, refractive, MIGS, dry eye therapies). The challenge isn’t that patients don’t care about vision—it’s that they often can’t convert what you said into a decision they feel confident living with.
Patients don’t decide based on what you know. They decide based on what they see, feel, and can repeat back.
The two “yeses”
- Clinical acceptance: “I get it, it matters, and I want the treatment.”
- Financial acceptance: “I can execute the plan without confusion or panic.”
The mistake most practices make is trying to “fix” weak clinical acceptance with a strong financial conversation. That’s backwards. The belief is created in the exam lane. The rest should feel like execution.
Clinical Acceptance 101 Proof → Meaning → Path
If you want a scaffold (not a pot of knowledge), keep the entire article anchored to three elements:
- Proof: show the patient what you see (in a deliberate order)
- Meaning: translate it into their life + what happens if they wait
- Path: make the next step simple and frictionless
Clinical acceptance is created by Proof + Meaning in the exam lane.
Financial acceptance is enabled by Path outside the exam lane.
If you believe a multifocal or EDOF lens will truly help this patient, the “value decision” has to happen in the exam lane—not at checkout.
That happens through anchoring: translating the lens from specs to their real life. Not “more range,” but night driving with less glare, reading menus without readers, seeing your phone at the store, working at a computer without constant glasses switching, traveling without multiple pairs.
Then pair the anchor with honest tradeoffs (halos, adaptation, who does well, backup plan). Do that, and patients leave thinking about scheduling—not whether you’re upselling them.
How to NOT get good clinical case acceptance – Talking about the wrong thing and skipping the anchor
What clinicians often say is medically accurate—but not decisional:
- “2+ nuclear sclerosis.”
- “RNFL thinning.”
- “Visually significant cataract.”
- “Candidate for toric IOL.”
- “We recommend SLT.”
Patients don’t decide based on labels. They decide based on outcomes they can picture and repeat back:
- “I want to drive at night without glare.”
- “I’m scared of losing independence.”
- “I can’t read menus and my phone without constant switching.”
- “I’m anxious because I don’t feel anything—but you’re telling me damage is happening.”
This is anchoring. Anchoring is the bridge: you connect the finding to a lived scene and a lived consequence.
Example (premium lens decision, anchored):
Not: “This lens gives more range.”
Instead: “This is the difference between night driving without fighting glare, reading menus without hunting for readers, seeing your phone at the grocery store, and working at a computer without switching glasses all day.”
Then pair anchoring with plain-language tradeoffs (patients can smell omission):
“Yes, halos can happen. Here’s who does well, who doesn’t, and what we do if you’re not perfectly glasses-free.”
That combination builds trust and lowers perceived risk.
Clinical Acceptance is Done in the Exam Lane. Part 1: Images: 5 Images, Shown in This Order
Dentistry solved case acceptance by turning the diagnosis into a repeatable visual experience—a handful of specific images, shown in a specific order, paired with a simple, consistent script. They even use AI to assist.
That approach translates perfectly to ophthalmology because we already have what most specialties wish they had: objective, visual proof (OCT, photos, fields, topography, glare testing). The problem isn’t lack of data. The problem is that we often show it randomly, explain it inconsistently, or bury the point in jargon.
The fix is simple: sequence the visuals and narrate them like a story—so the patient doesn’t just hear the diagnosis… they feel why it matters.
Here’s a practical ophthalmology version of that same “5–6 image” case acceptance system.1) Mirror Image: “This is your eye.”
Goal: credibility + attention
Use: the single most decisive image for that visit type (OCT, fundus photo, fields, topo, glare test, anterior segment photo).
Line:
“Before I tell you anything, I want you to see what I’m seeing. This is your eye—not a stock photo. I’m going to show you the one finding that matters most today.”
2) Scale Moment: “Where are you on the spectrum?”
Goal: self-identification (“Oh… I’m there.”)
Use: normal vs severe vs “you today” comparisons
- acuity + glare drop-off
- field progression examples
- optic nerve comparison
- mild → moderate → severe dry eye images (tasteful)
Line:
“Here’s what normal looks like, here’s severe, and here’s where you are today.”
3) Annotation Layer: “Make the invisible obvious.”
Goal: remove ambiguity
Use: simple highlighting/circling to direct the eye to the one key finding
Line:
“I’m going to highlight the exact spot so your eye goes straight to it.”
4) Consequence Image: “What happens if we ignore it?”
Goal: informed consent without fear-mongering
Use: appropriate stage-progression visuals (early → mid → late)
- advanced glaucoma field loss examples
- diabetic retinopathy progression
- wet AMD scarring examples
- cataract progression impacts (driving, falls risk, function)
Ethical framing line:
“This is not where you are today. I’m showing you the direction this can go if we do nothing—so you can make an informed decision.”
(Then stop talking for a beat.)
5) Options Map: “Here are the paths.”
Goal: convert belief into an actionable choice
Use: 2–3 options max, mapped to values (standard vs enhanced vs premium)
Line:
“Based on what you told me matters most—here are the options people choose, and what each one gets you.”
Part 2: The Words That Work: Concern → Movie → Plan
Images without narrative become confusion. Narrative without images becomes skepticism. Use a repeatable three-part script:
- Concern
“You have ___, and I’m concerned because ___.” - Movie (early → late)
“Right now, it’s like ___.”
“If we do nothing, what tends to happen is ___.”
“Over time, that can lead to ___.” - Plan
“The good news is ___.”
“Here’s what we do next ___.”
“Timing matters because ___.”
Then a pause that forces the real “yes” to form:
“What questions do you have before we talk about the options?”
Make It a Machine: Team Roles That Protect the “Yes”
High case acceptance scales when each role does a clean job—without stepping on the next person.
Player 1: The tech (pre-frame the anchor)
Give the doctor a simple, decisional snapshot (not just data):
- chief complaint in patient language (“night glare,” “can’t read,” “dry all day”)
- what they care about most (driving/reading/work/sports)
- anxieties (surgery fear, cost fear, prior bad experience)
- “seems ready / confused / resistant”
- tests completed
Two rules that protect trust:
- Don’t casually contradict your team in front of the patient. Reframe instead:
“I’m glad my team flagged this—here’s what I’m seeing after reviewing it closely.” - Praise your team out loud. Patients borrow confidence from how you treat staff:
“My technician did a thorough workup—this is exactly why we do these scans.”
Player 2: The doctor (create belief in the exam lane)
Your job is Proof → Meaning → Path. Not a lecture. Not jargon. A decision.
Player 3: The counselor/coordinator (execute, don’t “close”)
By the time a patient leaves the exam lane, they should already understand:
- the diagnosis
- the consequence of waiting
- the outcome goal
- the next step
Now the counselor handles:
- which option they chose
- what insurance covers vs elective
- payment paths
- paperwork
- dates offered now (momentum protected)
This separation makes the practice feel medical, not retail.
Financial Physics: Make Execution Easy
Once the patient believes, money should feel like planning—not persuasion.
What works consistently:
- Structure before number: “Most patients choose one of three paths…”
- Good / better / best (mapped to values): standard coverage vs upgraded function vs lifestyle-maximizing choice
- Clarity on coverage: “This portion is covered; this portion is elective.”
- Reduce friction immediately: schedule while motivation is alive, give a one-page summary, remove “call us later” gaps
- Translate complexity into a clean next step: “Here’s what happens next, and here’s what you do today.”
How to Measure Leaks (so this becomes operational)
If you want this to run like an operating system, measure where belief or momentum is breaking.
Track the funnel by step (weekly/monthly)
- Recommended → scheduled same day (by condition and by provider)
- Recommended → “think about it” rate (and the stated reason)
- Scheduled → completed (no-show/cancel rate)
- Premium option selection rate (for appropriate cohorts, not as a vanity metric)
- Time-to-schedule (days from exam lane recommendation to booked date)
Diagnose the leak by category
- High “think about it” after glaucoma education → weak Scale/Consequence step
- High premium interest but low conversion → anchoring/tradeoff framing inconsistent in exam lane
- High acceptance but low scheduling → counselor workflow / friction problem (not a doctor problem)
- Provider-to-provider variation → system inconsistency (images/script/order), not “personality”
Add one simple reason code
Require staff to tag “think about it” into 4–6 buckets:
- didn’t understand / confused
- fear of surgery
- cost / affordability
- needs spouse/family input
- time/logistics
- wants second opinion
Now you can fix the machine instead of guessing.
Closing Thought: Clinical Acceptance Is Patient Protection
Case acceptance isn’t about getting patients to do more. It’s about ensuring patients don’t drift into preventable harm because the practice failed to communicate clearly and keep momentum.
Win the clinical “yes” in the exam lane with Proof → Meaning → Path, and the rest becomes what it should be: calm logistics that help the patient act on a decision they already made.
Remember to review the entire module in order.
We talked about scheduling to optimize clinic flow and phone scripts to get your clinic busy.
Next we will dive deeper into financial acceptance.
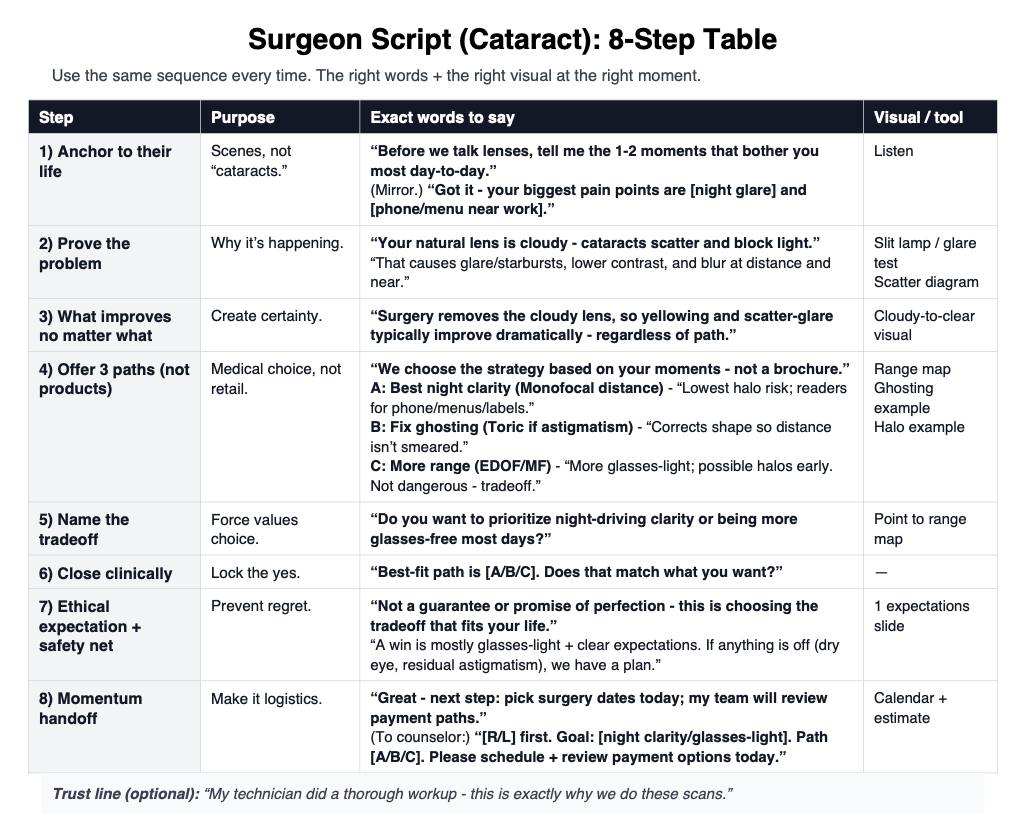
Here is my cheat cheat.
Page 1 is for your team
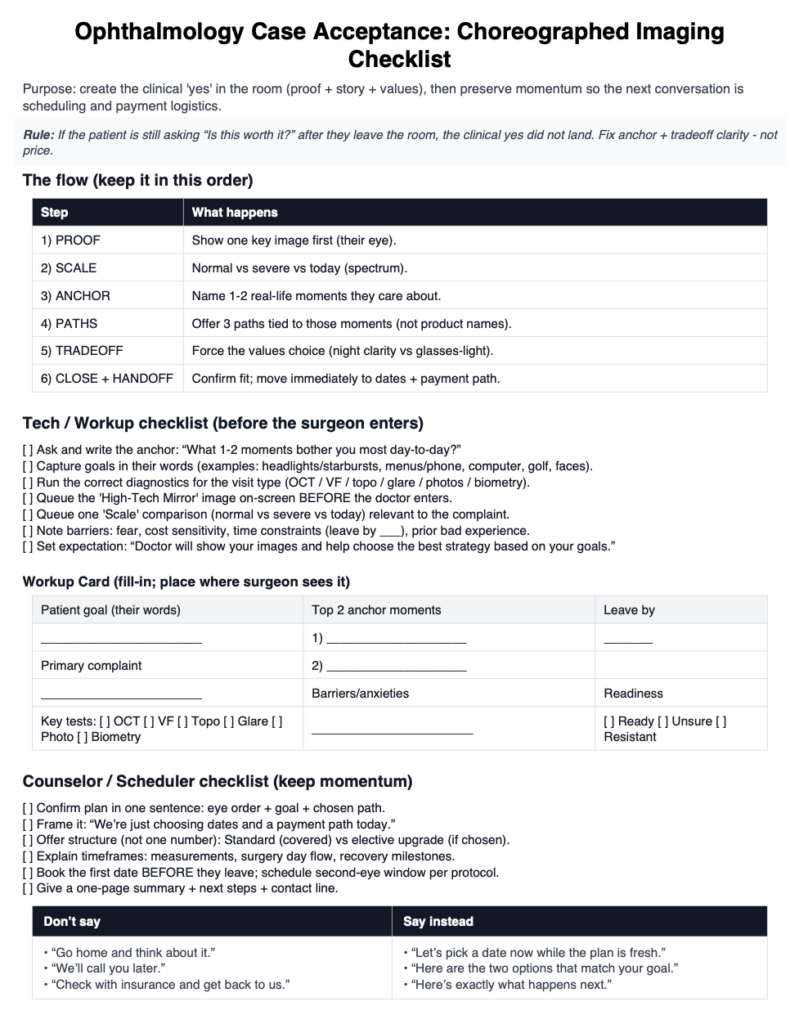
Page 2 is for you.

Pingback: Financial Case Acceptance: The One-Sheet Script That Works